Of all the major variables a person can change in their own health, cardiorespiratory fitness has the largest, most consistent link to how long they live. The signal is decades old and survives every adjustment thrown at it.
What the number means
VO₂max is the amount of oxygen the body uses per minute at maximum effort, divided by body weight. It depends on the lungs, heart, blood vessels and muscles all doing their job. No single organ owns it — it is a summary of physiological reserve.
The evidence is blunt: a low VO₂max raises the risk of dying earlier more than smoking does. In Mandsager's study of 122,007 patients, the least fit had roughly five times the mortality risk of the most fit — a wider gap than between smokers and non-smokers. It is the single most consequential variable a person can move.
A low VO₂max raises the risk of dying earlier more than smoking does.
Where the gains live
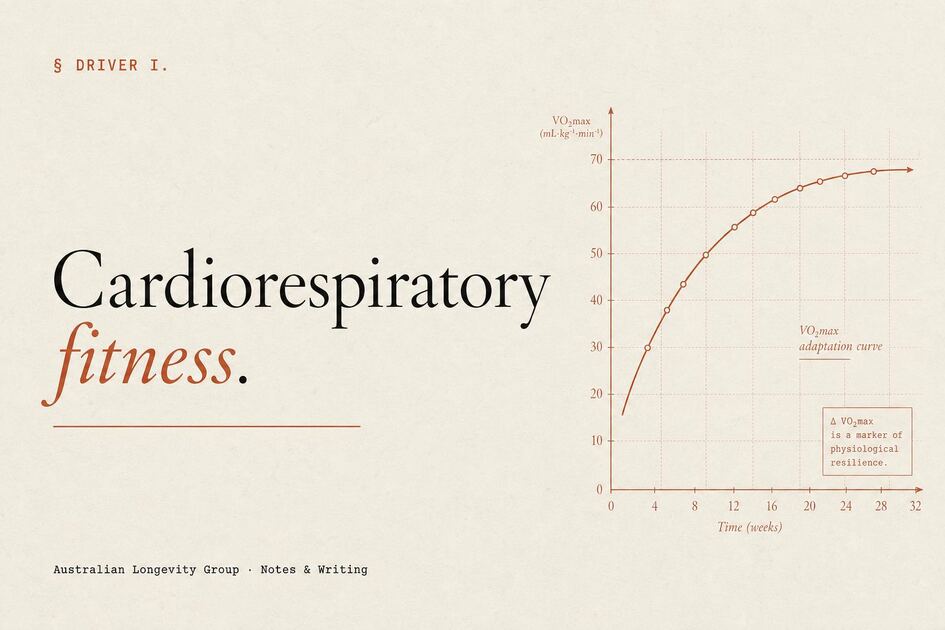
The curve is steep at the bottom and flat at the top. The biggest mortality drop sits between the least fit and the second-least fit. Going from sedentary to lightly active matters more than going from well-trained to elite. Unflattering to the marketing; useful for the patient who has not begun.
At the top end the picture is more nuanced than it is often presented. Very high lifetime endurance volumes are not obviously benign. Imaging in masters endurance athletes shows higher coronary artery calcium, more atrial fibrillation, patterns of myocardial fibrosis, and right-ventricular changes that do not always reverse with rest. The evidence here is smaller than at the low-fitness end, but the signal is real. The curve almost certainly flattens, and probably bends back, well before the volumes seen in elite ultra-endurance sport.
How it is built
The most effective mix in healthy adults is polarised: about 80% of weekly time at conversational pace (zone 2), and 20% at genuinely hard effort. Stöggl and Sperlich's 2014 trial in trained endurance athletes found this approach produced the biggest VO₂peak gain (+11.7% over nine weeks) of any model tested.
The most reliable hard-effort protocol is the Norwegian 4×4: four bouts of four minutes at 90–95% of max heart rate, with three minutes of easy recovery between, two or three times a week. In Helgerud's original cohort it produced a 7.2% rise in VO₂max in eight weeks; calorie-matched moderate or threshold work did almost nothing. Across the literature, longer intervals (two minutes or more, around fifteen minutes of hard work per session) beat short sprints and steady moderate work for VO₂max gain per unit of time.
The first three months of training expand the heart's pumping capacity. Plasma volume rises within hours and is sustained, red cell mass expands over weeks, and stroke volume goes up as the heart fills and empties more efficiently. Most of the early VO₂max gain is in the heart, not the muscle. The muscle's own oxygen-using machinery accrues over months and years, and matters more as training matures and as the body ages. This is why fitness drops fast in the first month of detraining — much of it is lost blood volume — and why two well-targeted sessions a week are enough to maintain peak fitness in older adults (Generation 100, in adults aged 70–77).
For a patient starting from a low base, the sequence usually runs: build a zone-2 base for two to three months until weekly volume tolerates 3–5 hours; add one 4×4 session a week; progress to two; layer in heavy resistance training for muscle, bone, and submaximal economy (no meaningful interference with VO₂max at normal doses). Modality matters less than adherence — cycling, rowing, running, swimming, brisk uphill walking, cross-country skiing all count. The best one is the one a patient will still be doing in five years. The same logic applies on the resistance side; see the companion note on strength and muscle.
What is worth measuring
A formal cardiopulmonary exercise test gives the cleanest reading. For most adults, a submaximal field test or wearable estimate is enough to track direction. Direction matters more than the absolute number — the question is whether the line is moving the right way over years.
The case for starting late
A common worry in the fifties and sixties is that the window has closed. It has not. Trainability is well preserved in later life, the relative gains can be large, and the absolute risk reduction from moving from low to moderate fitness in this group is among the biggest documented in preventive medicine. The work is not glamorous, but the dividend is real — and it compounds with the gains available from sleep and nutrition.
§ For professionals — mechanisms & evidence+
Mandsager and colleagues' retrospective cohort of 122,007 adults referred for treadmill testing at the Cleveland Clinic showed adjusted all-cause mortality falling stepwise across fitness categories, with hazard ratios for low-fitness adults comparable to or exceeding those associated with smoking, diabetes, and end-stage renal disease — and, notably, no observed upper limit of benefit at the extreme-fitness end of the distribution 1. Kokkinos' Veterans Exercise Testing Study cohort replicated the gradient across age, sex, and racial subgroups 2.
The Copenhagen Male Study and FRIEND registry data converge on a roughly 10–15% reduction in all-cause mortality per 1-MET increment in objectively measured fitness, persistent after adjustment for traditional risk factors 3,4. Mechanistically, higher cardiorespiratory fitness correlates with improved endothelial function, mitochondrial density, lower resting sympathetic tone, better insulin sensitivity, and reduced ectopic fat deposition.
Practical translation
Meta-analytic ranking for VO₂max gain in healthy adults places long-interval HIIT (≥2 min bouts, ≥15 min/session, 4–12 weeks) and polarised 80/20 distributions ahead of short-interval HIIT or SIT, with matched-work moderate-intensity continuous training (MICT) consistently inferior in head-to-head trials (Wen 2019; Milanović 2015; Bacon 2013; Stöggl & Sperlich 2014). The Norwegian 4×4 at 90–95% HRmax, three sessions per week over eight weeks, produced a 7.2% VO₂max gain in Helgerud's original cohort with no significant change in iso-caloric MICT arms 5; Wisløff's heart-failure trial showed +46% VO₂peak vs +14% MICT with LV reverse remodelling.
Central adaptations — plasma-volume expansion, stroke volume, peak cardiac output — dominate VO₂max gains over the first 6–12 weeks (Montero 2015; Lundby 2017). Peripheral adaptations (mitochondrial density, a-vO₂ difference) accrue over months to years and increasingly protect VO₂max with ageing. Two 4×4 sessions per week were sufficient to prevent the expected five-year decline in VO₂peak in adults aged 70–77 in Generation 100 (Stensvold 2020), and Hickson & Rosenkoetter established 2 d/wk at preserved intensity as the empirical minimum for maintenance.
A defensible starting prescription for most untrained adults: a polarised base of three to five hours per week of zone-2 conversational aerobic work, with one to two long-interval HIIT sessions (4×4 or equivalent) layered in once tolerance is established. Heavy resistance training is complementary rather than competing — interference effects on VO₂max are not seen at typical doses, and improved economy raises usable fraction of VO₂max at submaximal workloads. The American Heart Association's scientific statement frames objectively measured VO₂max as a clinical vital sign worth obtaining when feasible 6.
The Australian Physical Activity and Sedentary Behaviour Guidelines recommend 150–300 minutes of moderate or 75–150 minutes of vigorous activity per week, with muscle-strengthening on at least two days. The longevity literature suggests the upper end of these bands, not the lower, is where the cardiovascular dividend lives.
The extreme-volume question
The concern that very high lifetime endurance volumes may be net-detrimental to cardiac health is, in clinical practice, not trivial. Imaging studies in masters endurance athletes show consistent signals of increased coronary artery calcium burden, higher prevalence of atrial fibrillation, myocardial fibrosis on cardiac MRI, and right-ventricular remodelling that does not always normalise with detraining. The literature is smaller and less tidy than the dose-response data at the low-fitness end, but it should not be dismissed. The clinically interesting band for most patients is well below the volumes at which these signals appear; the message is not "more is always better" but "the dose-response curve flattens long before recreational athletes reach the volumes that raise legitimate concern".
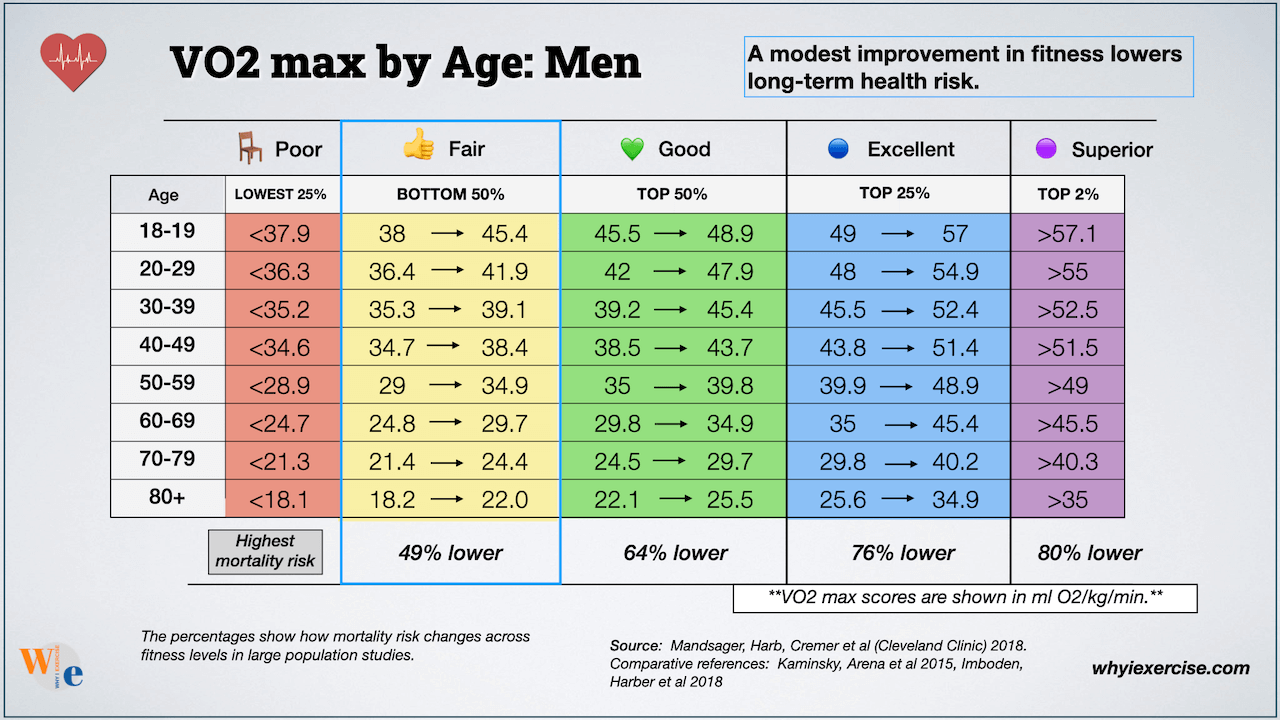
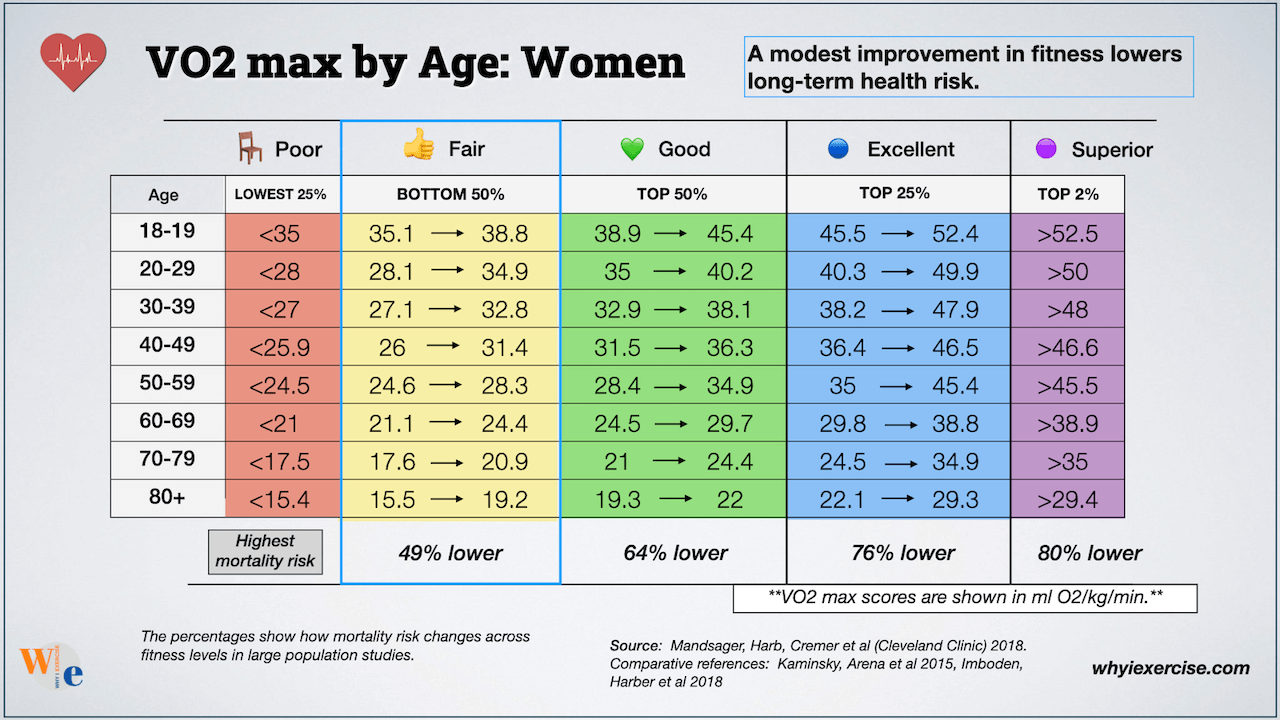
What VO₂max should I aim for at my age?+
Reference values vary by age and sex. Sitting in the upper half of your age band — the Good bracket or higher in the tables below — is associated with substantial reductions in all-cause mortality, with the curve continuing to bend favourably as fitness rises. The clinically interesting figure is rarely a single reading but the direction of travel year on year.
Is it too late to improve cardiorespiratory fitness in my fifties or sixties?+
No. Trainability is preserved well into later decades, and the absolute risk reduction from moving out of the lowest fitness quintile is among the largest documented in preventive medicine. Most adults who start late see meaningful gains within three to six months of consistent training.
How much zone-2 work do I actually need?+
For most untrained adults, three to five hours per week of conversational-pace aerobic work, supported by one or two shorter higher-intensity sessions, is a defensible starting point. Volume is progressed gradually. Adherence over years matters more than the specific weekly total.
Do I need a clinical VO₂max test, or is a wearable enough?+
A formal cardiopulmonary exercise test gives the cleanest reading and is worth obtaining periodically when feasible. For routine tracking, a submaximal field test or wearable-derived estimate is sufficient to follow direction. The clinical question is rarely the absolute number; it is whether the line is moving the right way.
- 1. Mandsager K, et al. Association of cardiorespiratory fitness with long-term mortality among adults undergoing exercise treadmill testing. JAMA Network Open. 2018.
- 2. Kokkinos P, et al. Cardiorespiratory fitness and mortality risk across the spectra of age, race, and sex. Journal of the American College of Cardiology. 2022.
- 3. Schnohr P, et al. Various leisure-time physical activities associated with widely divergent life expectancies: the Copenhagen City Heart Study. Mayo Clinic Proceedings. 2018.
- 4. Kaminsky LA, et al. Reference standards for cardiorespiratory fitness measured with cardiopulmonary exercise testing: data from the FRIEND registry. Mayo Clinic Proceedings. 2017.
- 5. Wisløff U, et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients. Circulation. 2007.
- 6. Ross R, et al. Importance of assessing cardiorespiratory fitness in clinical practice: a case for fitness as a clinical vital sign. Circulation. 2016.
- 7. Australian Government Department of Health. Physical Activity and Sedentary Behaviour Guidelines for Adults.