Of the things a person can change, sleep is the one most often written off and most often, in retrospect, the lever. The literature is large, the consensus on the basics is durable, and the cultural willingness to take it seriously is still catching up.
Three numbers worth knowing
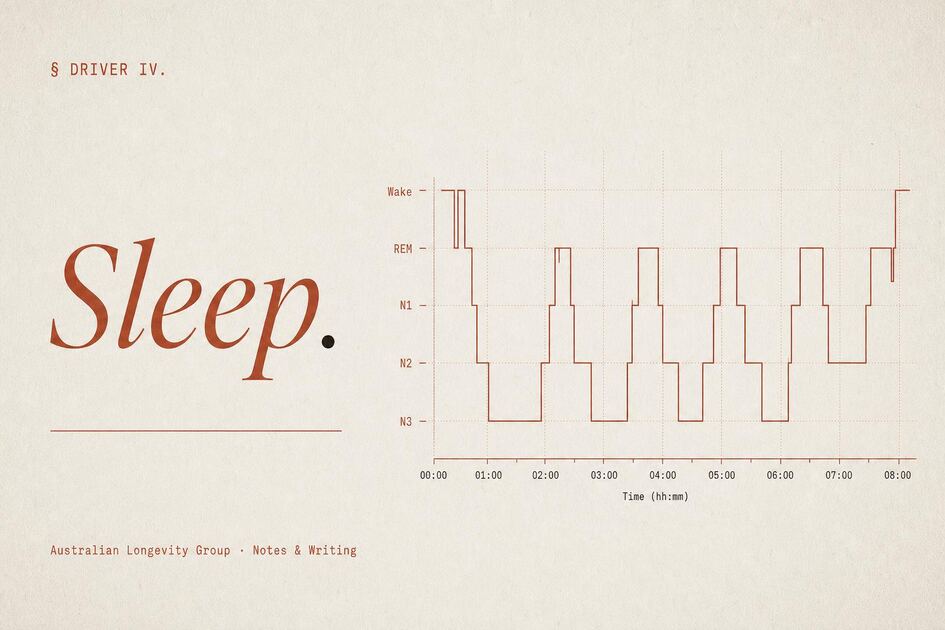
Regularity, architecture, and duration. The public conversation still revolves around duration. Inside the literature, regularity is now understood to be at least as informative, and architecture — the proportion of the night spent in deep and REM sleep — predicts cognitive trajectories in ways shorter summary measures do not.
Duration, briefly
The mortality curve against sleep duration is U-shaped and bottoms out near seven hours for most adults. Both routine short sleep and routine long sleep are associated with worse outcomes, though the long-sleep tail is harder to read and likely reflects subclinical illness as much as anything causal. The headline is unspectacular: aim for the middle, defend it.
Regularity is the underrated one
A person who sleeps the same hours every night does better on hard endpoints than a person who averages the same total but ranges widely. In the UK Biobank accelerometry cohort, regularity predicted all-cause, cardiovascular, and cancer mortality after adjustment for total duration — in several analyses more strongly than duration itself. The useful operational question is rarely how long did you sleep last night; it is how close was last week to the week before.
Architecture and the brain
The proportion of the night in REM and deep sleep is not a curiosity. In the Framingham cohort, a lower share of REM sleep independently predicted dementia incidence over twelve years; more recent blood-marker work links a delayed first REM episode to early Alzheimer's changes before symptoms appear. The brain has its own overnight clearance system that removes metabolic waste, and it runs preferentially during sleep. The mechanism is still being mapped, but the direction is consistent: sleep does structural maintenance, and disturbed nights interrupt it.
The undiagnosed apnoea problem
Obstructive sleep apnoea is one of the most clinically consequential conditions in Australian adults that goes unidentified. Australian cohorts suggest moderate-severe disease in roughly one in five middle-aged men, with around four in five cases undiagnosed across the broader population. The classic picture — middle-aged, snoring, daytime somnolence, modest abdominal adiposity — only captures part of those affected. Lean adults with narrow airways, women in midlife and after menopause, and adults with treatment-resistant hypertension are all systematically under-screened. A validated questionnaire and an Epworth score are the entry point; the threshold for a sleep study should be low.
What treatment actually looks like
CPAP remains the reference treatment for moderate-to-severe disease and reliably improves symptoms, mood, and blood pressure. The cardiovascular event reduction once assumed to follow has not been cleanly shown in randomised trials, and adherence — most patients tolerate the mask for fewer hours than the trials assumed — accounts for much of the gap. Mandibular advancement splints (a custom mouthpiece that holds the lower jaw forward overnight), weight loss, a small implanted nerve stimulator in selected anatomy, and side-sleeping approaches each have a place. Tirzepatide has recently shown a substantial reduction in apnoea events in obese patients with sleep apnoea, which expands the toolkit rather than replacing the mask.
What the bedroom is doing
Cool, dark, quiet. Bedrooms above the low twenties Celsius reliably degrade sleep quality. Light in the hour before bed, especially short-wavelength, suppresses melatonin and shifts circadian phase, with wide inter-individual variation in sensitivity. Caffeine taken six hours before bed measurably shortens total sleep time even when the person feels unaffected. Alcohol fragments sleep architecture in a dose-dependent way, with effects long after the person feels sober. Late, large meals do similar damage. None of this is hard to act on; most of it is not acted on.
Pharmacology is a poor first line
For chronic difficulty sleeping, the strongest evidence — and the only intervention with a strong recommendation in the current American Academy of Sleep Medicine guideline — is cognitive behavioural therapy for insomnia. It outperforms most pharmacological options on durable outcomes and does not accumulate the cognitive, falls, and dependence risks that benzodiazepines and Z-drugs carry, particularly past sixty-five. The newer dual orexin receptor antagonists are a real improvement on older classes. In Australia, low-dose modified-release melatonin is available through pharmacists for short-term use in older adults. None of these displace the behavioural work as the foundation.
What it costs to ignore
A decade of compressed, irregular sleep is not paid in tiredness. It is paid in cardiovascular risk, glycaemic control, mood, immune function, and the cognitive trajectory of later life. Of the levers in preventive medicine, this is among the cheapest to pull and the most often left alone — and it sits upstream of much of what is treated separately as stress and resilience and cardiorespiratory fitness.
§ For professionals — mechanisms & evidence+
All-cause mortality describes a U-shaped curve against habitual sleep duration with a nadir at approximately seven hours per night. The Cappuccio meta-analysis of sixteen prospective cohorts (n ≈ 1.38 million) reported pooled relative risks of 1.12 for short sleep and 1.30 for long sleep 1; the Yin pooled analysis of roughly 3.5 million participants reproduced the shape, with mortality rising by ~6% per hour below seven and ~13% per hour above 2. The long-sleep tail attenuates substantially when stratified by health status and is best read as a marker of subclinical disease rather than a causal exposure.
Sleep regularity now sits alongside duration as an independent — and in several analyses stronger — predictor of hard endpoints. In Windred's UK Biobank accelerometry cohort (n = 60,977, >10 million hours), quintiles 2–5 of the Sleep Regularity Index carried 20–48% lower all-cause mortality, 16–39% lower cancer mortality, and 22–57% lower cardiometabolic mortality versus the lowest quintile, adjusted for total sleep duration 3. Yiallourou and colleagues extended the signal to incident dementia and reduced brain volume 4.
Architecture and cognitive risk
REM and slow-wave sleep both contribute to glymphatic clearance and memory consolidation. In the Framingham cohort, each one-percent reduction in REM proportion carried a 9% increased hazard for incident dementia over 12 years; NREM stages were not predictive 5. Leng's plasma biomarker work links delayed REM latency to higher p-tau181 and amyloid-PET positivity, and Ohayon's meta-analysis describes a linear 2% per-decade decline in slow-wave sleep through mid-adulthood that plateaus after sixty 6.
Obstructive sleep apnoea
OSA is the single most consequential under-diagnosed sleep condition in Australian adults. The MAILES cohort placed moderate-severe prevalence in men aged 40–69 at 20.3%; the Busselton Healthy Ageing Study reported AHI ≥5 in around half of adults 46–65; an estimated 80% of cases remain undiagnosed 7. Untreated severe OSA carries an approximately threefold cardiovascular mortality signal in observational cohorts 8.
CPAP improves symptoms, mood, blood pressure, and quality of life, but the SAVE trial — 2,717 adults with established cardiovascular disease and moderate-severe OSA followed for 3.7 years — did not show a reduction in major cardiovascular events at a mean adherence of 3.3 hours per night 9. Subsequent pooled analyses suggest benefit emerges when adherence is robust and patient selection is appropriate. Mandibular advancement splints, hypoglossal nerve stimulation in selected anatomy, weight loss, and positional therapy each occupy defined niches.
SURMOUNT-OSA (Malhotra 2024) is the most significant recent shift: at 52 weeks, tirzepatide reduced AHI by 25–29 events per hour versus placebo in adults with moderate-severe OSA and obesity, both with and without concurrent PAP, alongside reductions in hypoxic burden, hsCRP, systolic blood pressure, and body weight 10. It does not replace CPAP in all phenotypes, but it materially expands the toolkit in the obese OSA phenotype.
In Australia, GP-initiated referral for an MBS-rebated Level 1 polysomnogram (Item 12203) requires a validated screening questionnaire (STOP-Bang ≥3, OSA50 ≥5, or high-risk Berlin) together with an Epworth Sleepiness Scale ≥8. Austroads' Assessing Fitness to Drive (2022) sets out the licensing implications of established sleep apnoea syndrome and sleepy-driving history; conditional licensing typically requires documented CPAP adherence around four hours per night.
Insomnia and pharmacotherapy
CBT-I is the only intervention carrying a STRONG recommendation in the 2021 AASM clinical practice guideline for chronic insomnia and is endorsed first-line by the American College of Physicians and the RACGP HANDI. Trauer's meta-analysis (20 RCTs) reported reductions of 19 minutes in sleep-onset latency, 26 minutes in WASO, and a 9.9-point gain in sleep efficiency, with durable effect at follow-up 11. Digital delivery (Sleepio, SHUTi) reproduces clinically meaningful effects and extends reach.
Among pharmacological options, the dual orexin receptor antagonists (daridorexant 50 mg, lemborexant, suvorexant) outperform older hypnotics on objective PSG endpoints without next-day sedation in published trials. Z-drugs and benzodiazepines carry an "avoid" designation in the 2023 AGS Beers Criteria for adults ≥65, with Glass's meta-analysis quantifying roughly fivefold odds of cognitive adverse events against a sleep-time gain of about 25 minutes 12. In Australia, modified-release melatonin ≤2 mg has been Schedule 3 for short-term monotherapy of primary insomnia in adults ≥55 since June 2021; evidence in adult sleep-maintenance insomnia remains modest, with the strongest signal in circadian rhythm disorders and older adults with low endogenous secretion.
Behavioural and circadian inputs
Tasali's 2022 trial in habitually short-sleeping adults with overweight demonstrated that a single sleep-extension counselling session increased nightly sleep by 1.2 hours and reduced caloric intake by approximately 270 kcal per day over two weeks — a tractable behavioural lever with metabolic consequence 13. Caffeine taken six hours before bed measurably degrades total sleep time; alcohol fragments architecture in a dose-dependent way; evening light exposure suppresses melatonin with marked inter-individual variability. Shift work carries a consistent coronary signal (Vyas 2012: pooled MI RR 1.23) and an IARC Group 2A cancer classification.
How many hours of sleep should an adult get?+
The mortality curve against sleep duration is U-shaped, with the nadir near seven hours per night for most adults. Both routine short sleep (under six hours) and routine long sleep (over nine) are associated with worse outcomes, though the long-sleep tail is harder to read and likely reflects subclinical illness in part. Aim for the middle of the band and defend it.
Is sleep regularity really more important than duration?+
In the UK Biobank accelerometry cohort of roughly sixty thousand adults, sleep regularity predicted all-cause, cardiovascular, and cancer mortality after adjustment for total duration — in some analyses more strongly than duration itself. The most useful operational question is rarely how long you slept last night; it is how close last week looked to the week before.
How do I know if I have sleep apnoea?+
The classic picture is loud snoring, witnessed pauses in breathing, daytime somnolence, and morning headaches, but the condition is significantly under-diagnosed in women, in lean adults with narrow airways, and in those with treatment-resistant hypertension. Australian estimates place around four in five cases as undiagnosed. Validated screening (STOP-Bang, OSA50, Berlin) combined with the Epworth Sleepiness Scale now enables GP referral for an MBS-funded sleep study.
Are sleeping pills a reasonable long-term solution?+
For chronic difficulty sleeping, cognitive behavioural therapy for insomnia (CBT-I) is the only intervention carrying a strong recommendation from the American Academy of Sleep Medicine and is endorsed first-line by the RACGP. Benzodiazepines and Z-drugs carry meaningful cognitive, falls, and dependence risk, particularly past sixty-five, and are not recommended for ongoing use. Newer dual orexin receptor antagonists are a real improvement on older classes but still sit beside, not above, the behavioural work.
What temperature should the bedroom be?+
Most adults sleep best in a room kept in the high teens to low twenties Celsius. Bedrooms above that reliably degrade sleep quality. Cool, dark, and quiet remain the three environmental variables most worth getting right.
- 1. Cappuccio FP, et al. Sleep duration and all-cause mortality: a systematic review and meta-analysis of prospective studies. Sleep. 2010.
- 2. Yin J, et al. Relationship of sleep duration with all-cause mortality and cardiovascular events: a systematic review and dose-response meta-analysis of prospective cohort studies. JAHA. 2017.
- 3. Windred DP, et al. Sleep regularity is a stronger predictor of mortality risk than sleep duration: a prospective cohort study. Sleep. 2024.
- 4. Yiallourou SR, Pase MP, et al. Association of sleep regularity with the risk of incident dementia and brain volume. Neurology. 2024.
- 5. Pase MP, et al. Sleep architecture and the risk of incident dementia in the community. Neurology. 2017.
- 6. Ohayon MM, et al. Meta-analysis of quantitative sleep parameters from childhood to old age in healthy individuals. Sleep. 2004.
- 7. Senaratna CV, et al. Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep Medicine Reviews. 2017.
- 8. Marin JM, et al. Long-term cardiovascular outcomes in men with obstructive sleep apnoea-hypopnoea with or without treatment with continuous positive airway pressure: an observational study. Lancet. 2005.
- 9. McEvoy RD, et al. CPAP for prevention of cardiovascular events in obstructive sleep apnea (SAVE trial). NEJM. 2016.
- 10. Malhotra A, et al. Tirzepatide for the treatment of obstructive sleep apnea and obesity (SURMOUNT-OSA). NEJM. 2024.
- 11. Trauer JM, et al. Cognitive behavioral therapy for chronic insomnia: a systematic review and meta-analysis. Annals of Internal Medicine. 2015.
- 12. Glass J, et al. Sedative hypnotics in older people with insomnia: meta-analysis of risks and benefits. BMJ. 2005.
- 13. Tasali E, et al. Effect of sleep extension on objectively assessed energy intake among adults with overweight in real-life settings: a randomized clinical trial. JAMA Internal Medicine. 2022.
- 14. Edinger JD, et al. Behavioral and psychological treatments for chronic insomnia disorder in adults: an American Academy of Sleep Medicine clinical practice guideline. JCSM. 2021.